Application of brain research in prescribing antidepressants successful
Nijmegen, January 26, 2021 – The success rate of antidepressants in the treatment of depression can be greatly improved thanks to the use of a short brain examination (EEG) prior to treatment. A study conducted in the Netherlands examined, for the first time, the use of EEG as a biomarker in practice.
[custom-twitter-feeds]
News archives
consensusverklaring
Paradigmaverschuiving binnen de psychiatrie: Standaarden voor magnetische hersenstimulatie bij depressie
Nijmegen, 18 juni 2019 –Na meer dan 30 jaar onderzoek naar transcraniële magnetische hersenstimulatie (rTMS) bij de behandeling van depressie, dringt deze techniek steeds verder door in de psychiatrische en psychologische behandelpraktijk. Om die reden hebben verschillende onderzoekers en instanties (waaronder Onderzoeksinstituut Brainclinics, NedKAD en de hersenstimulatiestichting) zojuist een consensusverklaring gepubliceerd in het tijdschrift voor psychiatrie. Deze verklaring dient ter verduidelijking van de rol en plek van magnetische hersenstimulatie bij de behandeling van depressie maar ook als handvat om deze techniek effectief en veilig toe te passen.
Noodzaak: de ontwikkeling van nieuwe antidepressiva stagneert.
Sinds 2010 investeren de meeste farmaceutische bedrijven niet meer in de ontwikkeling van nieuwe antidepressiva, waardoor er grote behoefte is aan nieuwe en effectievere behandelingen van depressie.
Magnetische hersenstimulatie: Een paradigmawisseling binnen de psychiatrie?
Binnen de psychiatrie wordt de techniek van transcraniële magnetische hersenstimulatie (rTMS) al sinds 1985 intensief onderzocht. Deze techniek is onderdeel van een bredere ontwikkeling binnen de psychiatrie, waarbij steeds meer aandacht is voor ‘neuromodulatie’ technieken, waarbij hersenactiviteit veel gerichter beïnvloed kan worden, vaak met minder bijwerkingen in vergelijking met medicatie. Voorbeelden van deze neuromodulatie technieken zijn onder andere diepe hersenstimulatie bij Parkinson, dwang en depressie, maar ook rTMS.
Het duurt vaak lang voordat dit soort nieuwe ontwikkelingen doordringt in de psychiatrische en psychologische behandelpraktijk, te vergelijken met de trage adoptie van de elektrische auto, en dit wordt binnen de psychiatrie dan ook gezien als een paradigmaverschuiving.
rTMS bij depressie en consensusverklaring
Dr. Martijn Arns is sinds 2006 één van de pioniers die zich heeft toegelegd op de toepassing en vooral verfijning en optimalisatie van de transcraniële magnetische hersenstimulatie techniek (rTMS), bij met name de behandeling van depressie. Sinds medio 2017 is deze behandeling ook erkend als vergoede zorg door Nederlandse zorgverzekeraars, waardoor meer patiënten profijt kunnen hebben van deze behandeling.
De belangrijkste conclusie van de consensusverklaring is dat rTMS een bewezen effectieve en veilige behandeling bij depressie is, met gunstige lange termijneffecten, mits de behandeling met rTMS wordt uitgevoerd onder supervisie van een (BIG) geregistreerde psycholoog of psychiater, waarbij de bekende veiligheidsrichtlijnen in acht worden genomen.
Martijn Arns: “Om die reden heeft een groep van onderzoekers van verschillende instanties en universiteiten, waaronder Onderzoeksinstituut Brainclinics, NedKad en de Hersenstimulatiestichting, de handen ineengeslagen om tot een eerste consensusverklaring te komen voor een veilige, verantwoorde en effectieve toepassing van rTMS bij de behandeling van depressie. Voor de kwetsbare patiëntgroepen die behandeld kunnen worden met rTMS is deze verklaring enorm belangrijk: het is een eerste aanzet tot standaardisering en kwaliteitsbewaking van (medisch) verantwoord handelen.”
Hoe werkt rTMS?
(repetitieve) Transcraniële magnetische stimulatie (rTMS) is een niet-invasieve en medicatie-vrije behandelmethode bij depressie. Een spoel die geplaatst wordt op het hoofd genereert een pulserend magnetisch veld en stimuleert specifieke gebieden van de hersenen die betrokken zijn bij depressie.
Na ongeveer 10 – 15 behandelsessies kunnen de eerste positieve effecten al waarneembaar zijn. In combinatie met psychotherapie kan dit effect worden versterkt en gestabiliseerd.
De behandeling is een precies gerichte, milde en veilige, effectieve therapie. Over het algemeen wordt de magnetische stimulatie niet als pijnlijk ervaren, maar een bijwerking van rTMS die soms voorkomt is lichte hoofdpijn. Deze wordt veroorzaakt door het samentrekken van spieren rondom hals, nek en hoofd en verdwijnt na korte tijd vanzelf.
rTMS is geschikt voor mensen met een depressie of behandelresistente depressie. rTMS werd voor het eerst succesvol toegepast in 1985. Sinds die tijd is de techniek uitgebreid onderzocht en steeds verder geperfectioneerd.
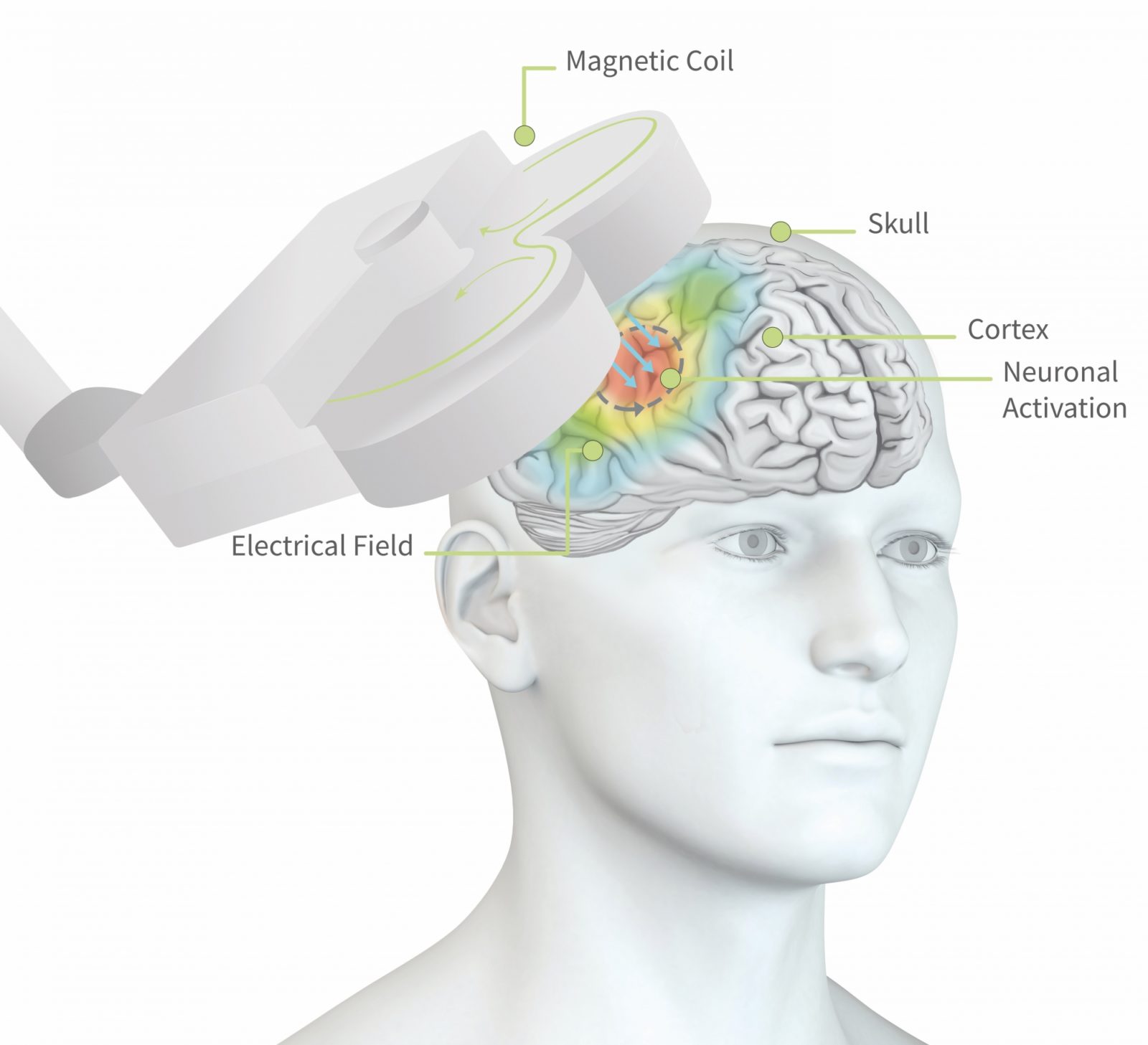
Figuur 1: de pulsen uit de magneetspoel dringen tot ca. 2cm diep in de hersenen door en stimuleren lokale hersencellen tot actie. Dit kan ervoor zorgen dat het groepje hersencellen, of het netwerk dat daaraan vast zit, geactiveerd wordt.
Referenties:
1)Arns, M., Bervoets, C., van Eijndhoven, P., Baeken, C., van den Heuvel, O. A., Aleman, A., . . . Sack, A. T. (2019). Consensusverklaring voor de toepassing van rTMS bij depressie in Nederland en België. Tijdschrift Voor Psychiatrie, 61(6), 411-420.
2) Donse, L., Padberg, F., Sack, A. T., Rush, A. J., & Arns, M. (2017). Simultaneous rTMS and psychotherapy in major depressive disorder: Clinical outcomes and predictors from a large naturalistic study. Brain Stimulation.doi: https://doi.org/10.1016/j.brs.2017.11.004
Lees de consensusverklaring
Zeven voor leven
Sponsoring groot succes
Het Brainclinics-Vidacto team droeg ruim duizend euro bij aan het totaal van €167.612,- dat de Zeven voor Leven sponsorrit bijeenbracht voor de Stichting Kanker Zien. Na afloop van de sponsorrit spraken we kort met Martijn Arns, oprichter van Brainclinics en ploegleider van het wielerteam.
Gefeliciteerd met jullie prestatie! Hoe ging het?
Dankjewel! Het viel 100% mee. De rit zelf was best stevig, 140 kilometer in totaal, en door het hoogteverschil van het parcours hebben we 2000 meters geklommen. De moraal was goed en bleef dat ook.
Hoe hoog eindigden jullie in het klassement?
Het mooie van de Zeven voor Leven sponsorrit is dat iedereen eigenlijk een winnaar is. De renners, die naar hun eigen maatstaf kunnen presteren, de sponsors, omdat ze bijdragen aan goed en belangrijk onderzoek naar het herkennen van kanker in een vroeg stadium, de Stichting Kanker Zien, omdat ze met een eerste sponsorrit al ruim 167.000 euro binnenhalen, en natuurlijk de (toekomstige) kankerpatiënten, die een betere overlevingskans in het vooruitzicht hebben.
Je noemt presteren naar je eigen maatstaf, wat bedoel je daarmee?
Een ronde is ongeveer 20 kilometer, en je kunt maximaal 7 ronden rijden. Maar omdat het sponsorbedrag niet verbonden is aan het aantal ronden dat je rijdt kan je ook minder ronden rijden en toch een vol bedrag binnenfietsen. Daardoor is meedoen eigenlijk belangrijker dan winnen, of veel kilometers maken. Ik ben blij met onze prestatie, we hebben met het team de zeven ronden volgemaakt en daarbij een goed gemiddelde gereden. En we hebben ruim duizend euro binnengebracht!
Volgend jaar weer?
Wie weet wat de toekomst brengt!

foto: Abigaël de Vries


Team Brainclinics-Vidacto. vlnr: Noud van Hecke, Bas Vroemen, Martijn Arns
The relationship between sleep and ADHD
Nijmegen, April 23rd, 2019 - Dutch researchers from Research Institute Brainclinics in Nijmegen and PsyQ, (Kenniscentrum ADHD bij volwassenen) in The Hague, discovered a striking link between light, sleep and ADHD, as can be read in two recent scientific publications. They published a study showing that ADHD can be a cause or a consequence of a disturbed sleep-wake rhythm. This new insight can be of great importance in the treatment of ADHD.
The importance of sleep
Three out of four adults and children (± 75%) with ADHD have difficulty falling asleep.
This sleep-wake disorder has major consequences for health, concentration and daily functioning: if you lie awake longer, you wake up less refreshed the next day, fatigue increases, and your school or work performance and concentration diminishes.
Circadian rhythm and sleep pressure
The orange line in Figure 1 shows how fatigue increases during the day. After you have slept, tiredness decreases. This is called sleep pressure. Ideally, sleep pressure and the biological clock are in sync.
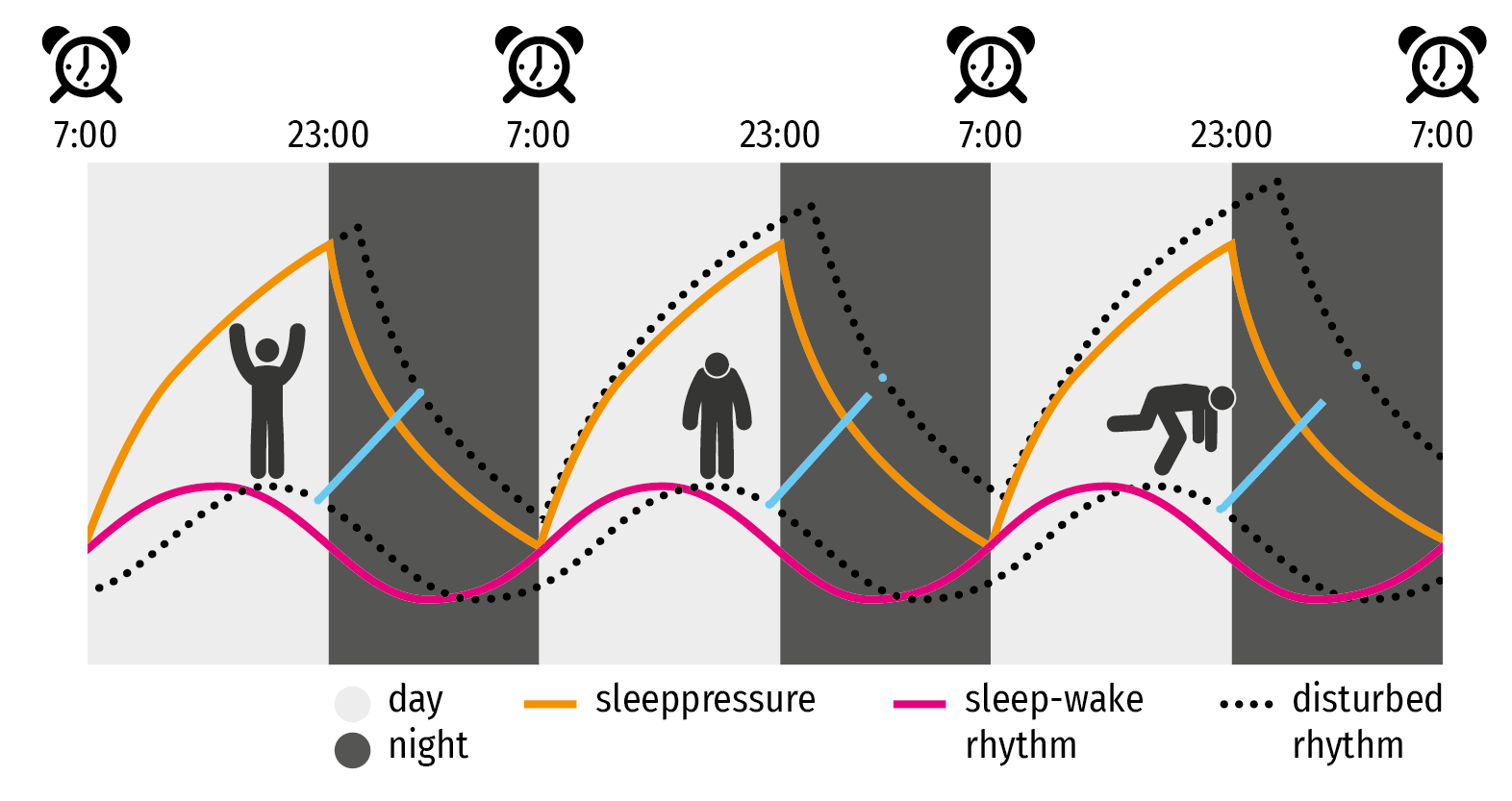
Figure 1: Circadian rhythm: With normal sleep, the ratio between sleep pressure (orange line) and circadian rhythm, also called biological clock, (pink line) is optimal. With a delayed rhythm, these processes increasingly grow further apart (blue lines): it becomes more difficult to fall asleep, and fatigue increases faster during the day.
How the circadian rhythm can be disturbed
Melatonin, the "sleep hormone", plays an important role in regulating the sleep-wake rhythm. The amount of melatonin your body releases is determined by the amount of daylight exposure. At the end of the day, when daylight decreases, you release more melatonin that makes you more sleepy assuming disturbing factors play no role. The use of modern media can be considered such a disturbing factor. Tablet and smartphone screens, but also LED lights, radiate blue light that falls in the same spectrum as daylight.If you use those in the evening, the body will postpone and lower the production of melatonin. The result: you will fall asleep later (sleep delay), and because your alarm clock (due to daily obligations) goes off at a regular time, you effectively sleep fewer hours.
The consequences of a (too) short night's rest (sleep restriction) are often underestimated, but the result of a few hours' missed sleep every night is comparable to staying awake for 48 hours (sleep deprivation), with all the associated negative effects. While the adverse effects of sleep deprivation are well known, with sleep restriction people are not aware of the same symptoms (for example, reduced concentration and vigilance).
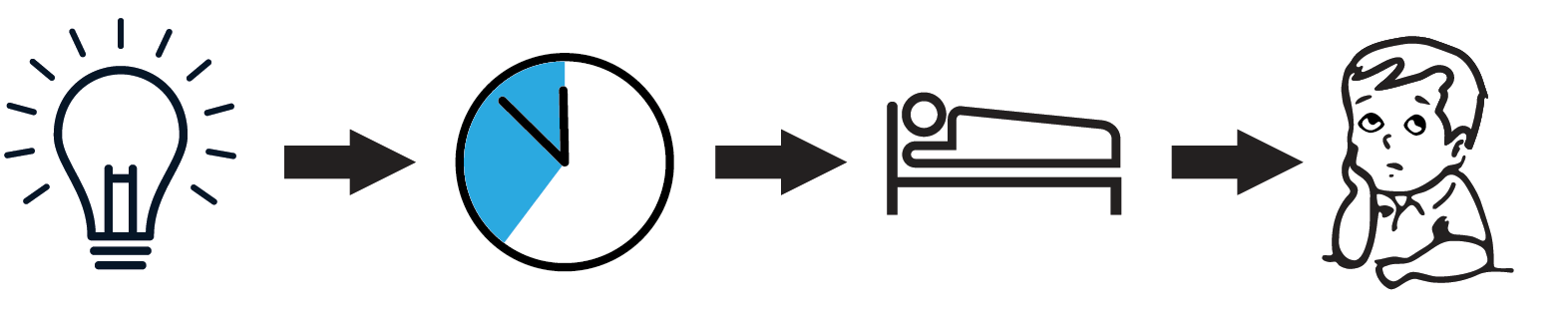
Figure 2: Consequence of exposure to blue light just before going to sleep: A pathway is depicted in which LED light exposure results in a sleep-onset delay, which in turn negatively influences the amount of time spent sleeping, which ultimately leads to worsening of attention.
Sleep problem as a cause and effect of ADHD
The functional and neuro anatomical overlap between brain areas involved in attention, alertness and sleep regulation reflects the complex relationship between ADHD and sleep.
A sleep problem can be either cause, effect or intrinsic characteristic of ADHD. An example: young children who are very tired become very energetic. Here, drowsiness is the cause of hyperactivity. However, ADHD can also be the cause of problems falling asleep: for example, problems with inner unrest, grinding, or pressure in the head. It could also be that ADHD and sleeping problems both stem from the same underlying problem.
Similarities between ADHD and sleep disorders
There are many similarities between the symptoms of ADHD and those of sleep disorders: problematic behavior, learning disabilities, concentration problems and emotion disorder, and often the symptoms of ADHD exacerbate the sleep problem, or vice versa. Symptoms of ADHD, a delayed circadian rhythm and sleep disorders are therefore intertwined. They seem to share a genetic and etiological background and can benefit from a common treatment.
How do you resolve sleeping problems?
Sleep problems related to mood or anxiety disorders can be reduced by addressing the causes. Sleep problems due to a chaotic lifestyle, which is generally a characteristic of ADHD, can be reduced by the medical and psychological treatment of ADHD itself. Improved sleep hygiene (no tablet or smartphone use in the hours before bedtime, no coffee in the evening, regular bedtimes) is very important. The preferred treatment for insomnia is a cognitive behavioral treatment (CBTi), which focuses on good sleep hygiene, good bed-sleep association and relaxation training, among other things. CBTi has been proven to be very effective for symptoms of insomnia and sleep quality improvement, is safe, has no side effects and is therefore preferable to sleep medication. Chronotherapy, for example through the administration of light therapy or melatonin, certainly has a positive effect on children with ADHD in the longer term, as has neurofeedback.
ADHD-SOM
Improving sleep quality has a favorable effect on ADHD symptoms and it is therefore advisable to include such a focus in ADHD treatments. In addition, the term ADHD is too general: because ADHD is so often associated with sleeping problems, the authors propose to create a separate DSM-5 classification for this category: ADHD-SOM (derived from somnus, or sleep), which enables specialists to propose a much more focused and personalized treatment.
References:
Bijlenga, D. Vollebregt, M.A. Kooij, J.J.S Arns, M. (2019) The role of the circadian system in the etiology and pathophysiology of ADHD: time to redefine ADHD?ADHD Attention Deficit and Hyperactivity Disorders DOI: 10.1007/s12402-018-0271-z
Arns, M. Vollebregt, M.A. (2019) Time to Wake Up: Appreciating the Role of Sleep in Attention-Deficit/Hyperactivity DisorderJournal of the American Academy of Child and Adolescent Psychiatry Vol.58 Number 4 April 2019 DOI: 10.1016/j.jaac.2018.10.013
racing against cancer
Nijmegen, 19 April 2019 - Brainclinics and Vidacto join forces to race towards a cancer-free future!
Zeven voor Leven (Seven for Life)
May 26, 2019, the cycling challenge Zeven voor Leven (Seven For Life) will be held for the first time in the hilly landscape around the municipality of Berg en Dal. The proceeds of the cycling round will go entirely to the Stichting Kanker Zien (Spot Cancer Foundation). The foundation wants to be able to diagnose cancer at an earlier stage and treat tumors in a more targeted way. This also improves the quality of life after treatment. The foundation even strives for complete prevention of this disease.
Frits Barend, Tim de Vries and Team Sunweb have committed themselves as ambassadors to Zeven voor Leven.
Trail
The trail is 20 km long and leads, among other things, along the Zevenheuvelenweg. The challenge is to complete the round seven times. During those 140 kilometers, around 2000 altimeters are made together. The start and finish take place at the Ketelwoud event site.

Route (subject to change)
Team Brainclinics-Vidacto
Team Brainclinics-Vidacto stands for health and vitality, and it is therefore a no-brainer for us to participate and thus contribute to this charity.
You can sponsor the Stichting Kanker Zien by visiting our team page and sponsoring us. In this way we all cycle to a future where cancer can be prevented!

Together towards a future in which cancer can be prevented!
Meta-analysis confirms sustained effects of neurofeedback
Meta-analysis confirms sustained effects of neurofeedback in children with ADHD
Nijmegen, February 16th, 2018 - An international group of researchers conducted a meta-analysis that systematically looked at all available studies and found that after an intensive course of neurofeedback, the clinical benefit of neurofeedback on ADHD symptoms was maintained over a 6-month follow-up period (without treatment). At follow-up the effects of neurofeedback were not inferior to active treatments such as medication, whereas benefits for non-active control groups (such as cognitive training) were no longer present at follow-up. These results have now been published in the scientific journal European Child & Adolescent Psychiatry.
Neurofeedback is a treatment where real-time feedback is provided on specific brain activity (most often the EEG) and based on learning principles participants learn to control specific types of brain activity. Based on the notion that this treatment is based on learning principles, it is expected that it should result in long-term benefits, however durability has not been systematically investigated. Given treatment with medication in ADHD is effective in short-term symptom management, and clinical benefit is likely to diminish after sustained use for more than 2 years, there is a need for treatments that result in better long-term benefits. Therefore, an international group of researchers from The Netherlands (Utrecht University, Research Institute Brainclinics, Radboud University), Germany (University Hospital Erlangen; kbo-Heckscher-Klinikum, Tübingen University, neuroCare Group), and the United States (UCLA), conducted a systematic-review and meta-analysis to investigate the long-term effects of neurofeedback and different control groups, including medication. This research group was selected to include scientists with different views on neurofeedback to interpret the data in a balanced and critical manner.
In this study, researchers compiled data of more than 500 children with ADHD comparing the results of neurofeedback, active (incl. medication), and 'non-active' control conditions from 10 randomized controlled studies (RCT's) and clinical benefit was assessed after a follow-up period of on average 6 months after treatment was finished. It was found that neurofeedback resulted in a large effect on inattention and medium effect on hyperactivity/impulsivity at follow-up and at this time-point there were no differences between neurofeedback and active-treatments. For non-active controls a small effect was found only on inattention that disappeared at follow-up. Numerically, the benefits of neurofeedback tended to improve from outtake to follow-up, which was not the case for the other treatments. Furthermore, for the medication groups, medication was still used in the 6 month interval to follow-up, whereas for neurofeedback no additional treatment sessions were administered in that interval.
Concluding, these results suggest that clinical benefits achieved with neurofeedback in children with ADHD have durable effects at least over a 6-month period without treatments, positioning neurofeedback as a promising treatment with long-term benefit.
Note: The results from this meta-analysis mainly apply to the specific protocols investigated and might not generalize to other 'experimental' approaches implemented in many 'neurofeedback clinics'. Currently, there is most consistent evidence for Slow Cortical Potential (SCP), Theta/Beta (TBR) and Sensori-Motor Rhythm (SMR) neurofeedback, see figure below for explanation.
Reference:
Van Doren, J., Arns, M., Heinrich, H., Vollebregt, M. A., Strehl, U., & Loo, S. K. (2018). Sustained effects of neurofeedback in ADHD: A systematic review and meta-analysis. European Child & Adolescent Psychiatry. doi:https://doi.org/10.1007/s00787-018-1121-4
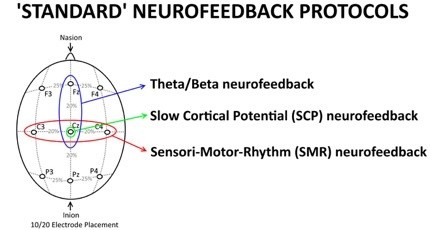
Figure 1 An explanation of 'Standard NF protocols' as a function of training site. Theta/Beta neurofeedback protocols are specifically trained at Fz or Cz, in line with most studies that have assessed the Theta/Beta ratio at those sites; SCP neurofeedback is always applied at Cz and SMR neurofeedback is always applied at a site that overlies the sensori-motor strip, i.e. C3, Cz or C4. Theta/Beta neurofeedback is focused on downtraining Theta and rewarding Beta, SMR is focused on SMR enhancement and SCP neurofeedback is focused on bidirectional training of negativation and positivation. These three protocols have been most investigated in the treatment of ADHD, and most studies included in the meta-analysis employed one of these protocols.
Male and female brain rhythms show differences
Male and female brain rhythms show differences; 'Deep-Learning' reveals different EEG patterns
The electric brain signals, measured by using EEG, of males and females show differences. The difference can’t be detected by visual inspection, not even by the trained eye of a neurologist. A ‘deep learning’ computer is able to find it. Researchers of the University of Twente, the University of Zürich and Research Institute Brainclinics in Nijmegen, publish these results in Scientific Reports of 15 February.
Male and female brains are different, functionally and anatomically. But that the EEG (electro-encephalography) signals, measured using electrodes placed on the skull, show different signals as well, was not demonstrated yet. For the interpretation of EEG signals, advanced pattern recognition techniques have been developed the last decades. Still, in many cases, the trained eye of the neurologist gives better results. Even these trained eyes are not able to recognize a difference between male and female brain rhythms. For this, artificial intelligence, so-called ‘deep learning’, is needed.
Training
The researchers had a large set of over 1300 EEG patterns, from several laboratories, at their disposal. This set has been entered into a learning computer, a so-called ‘convolutional neural network’. This is an artificial neural net existing of several layers and determining over nine million parameters. The network was first trained using 1000 EEG’s of just two minutes, with a known outcome: male or female. This was not a training based on entering specific characteristics, as these were not known beforehand. After training, the computer was fed with an independent set of EEGs. In over 80 percent, the system gives the right answer. This is well above the significance threshold.
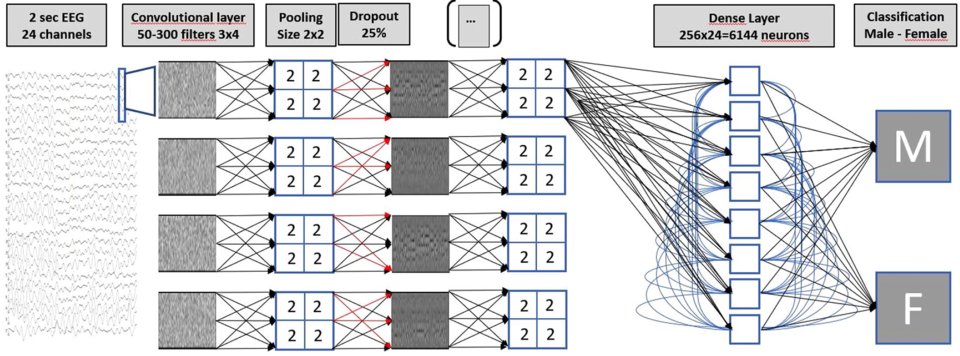
Figure 1 The multilayer neural net setup, used for classifying EEG readings
BETA ACTIVITY
The next step: extract the specific features that make the difference, from the neural net. The main difference is in the ‘beta activity’, a frequency range between 20 and 25 Hz. These rhythms have to do with cognition and with tasks that are emotionally positive or negative. It is known from previous research that females are better capable of recognizing emotion: this could indicate a difference in beta activity. Within the context of this research project, this has not been elaborated further. The outcomes don’t give an answer to transgender issues either.
PERSONALIZED TREATMENT
It seems a complicated way of assessing sex, using EEG and strong computing power. An interesting question, however, can be: do females and males respond to neurological or psychiatric disorders in different ways. And thus: is it, based on this knowledge, possible to better tailor the treatment? Apart from that, this research shows that there is a lot more information inside an EEG than meets the eye. Previous research using the combination of EEGs and deep learning, was on sleep analysis, responds to music or early detection of brain diseases. There is enough reason for further exploring this potential, as it could lead to better insights and personalized treatment.
The research has been done by Michel van Putten, professor of clinical neurophysiology at the University of Twente and neurologist at the Medisch Spectrum Twente hospital in Enschede. He collaborated with Sebastian Olbrich of the Psychiatric clinic of the University of Zürich and with Martijn Arns of Research Institute Brainclinics in Nijmegen. Also see University Twenthe website.
Their paper 'Predicting sex from brain rhythms with deep learning’, is published in ‘Scientific Reports’ of 15 february. This is a Nature publication.
Combined rTMS-psychotherapy effective treatment for depression
Combined rTMS and psychotherapy an effective treatment for depression
Nijmegen (The Netherlands), November, 16th 2017 – Magnetic brain stimulation (rTMS) combined with concurrent psychotherapy seems more effective, then either alone, as was just published in the international journal ‘Brain Stimulation’ based on a study in 196 patients. After an average of 21 sessions, 66% of patients with treatment resistant depression responded well to treatment, with a lasting effect after 6 months in 65% of this group.
rTMS an effective add-on for psychotherapy
A large study by Donse, Padberg, Sack, Rush and Arns 1), carried out in the Netherlands has investigated the effects of combining brain stimulation (rTMS) with concurrent psychotherapy in treatment resistant depression. The study was conducted by Research Institute Brainclinics in collaboration with neuroCare Group. The results of this study suggest that a combined approach is more clinically effective than if either therapy was delivered alone. 66% of the patients in this study responded positively to the combined therapy (i.e. symptom decrease of more than 50%), while 56% of the total sample achieved remission (meaning that they no longer met criteria for depression). Follow-up after 6 months demonstrated that 65% of the patients still had benefit from the initial course of treatment, which suggests that the effects are durable. On average patients received 21 treatment sessions. The results of this study are published this month in the leading international journal: Brain Stimulation.
Studies show that when either rTMS or Psychotherapy are conducted as a monotherapy, an average of 30-40% of patients achieve remission, clearly less than the 56% remission achieved with the combined treatment of rTMS and psychotherapy. Similarly, it is widely known that ‘psychotherapy and drugs’ combined show better outcomes, however this approach often requires two separate treatment programs and specialists, i.e. a Psychiatrist to deliver medications and a Psychologist to deliver Psychotherapy. A combined approach of Psychotherapy at the same time as brain stimulation, can be performed by one clinician and is shown to be more efficient, and above all, a more effective treatment for treatment resistant Depression.
Recognition
The efficacy of rTMS as a monotherapy (i.e. conducted without individual psychotherapeutic support) is recognized throughout the world as a valid treatment for Depression and is furthermore supported by FDA approval in the United States, and is recognized by NICE in the United Kingdom. Since 2011, Health Insurance providers in The United States, and more recently, in The Netherlands, reimburse rTMS treatment for treatment resistant depression.
How does it work, combined rTMS and Psychotherapy?
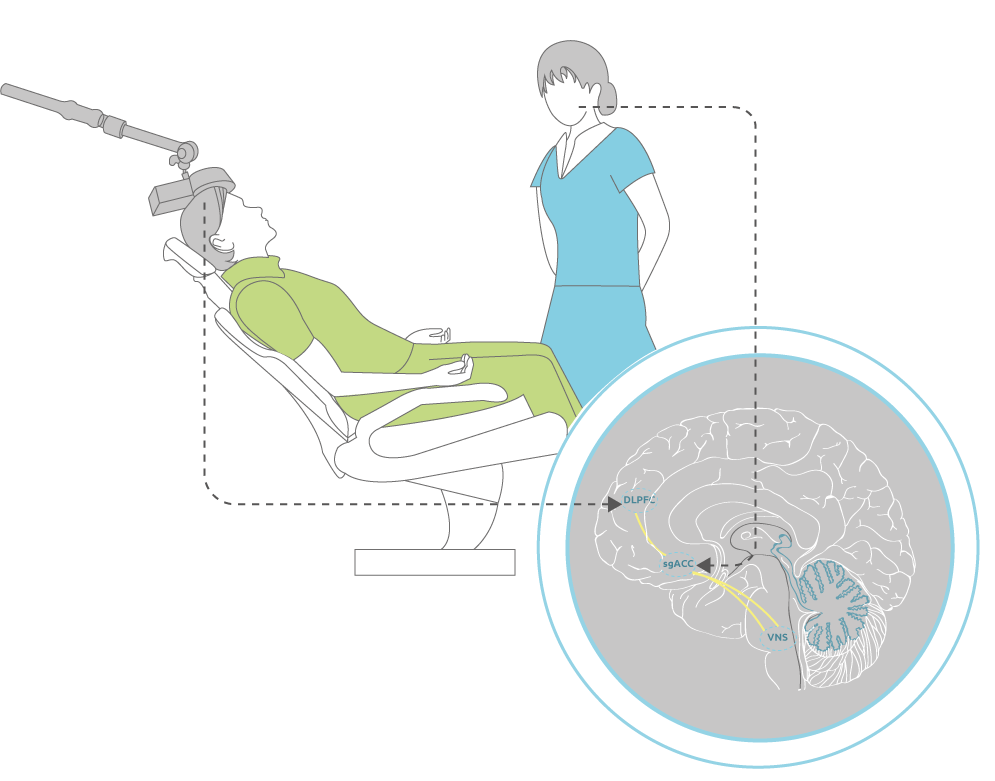
Research has shown that depression is linked to disrupted communication in a specific network of brain structures including the frontal cortex (dorsolateral prefrontal cortex (DLPFC)) and the deeper anterior cingulate (sgACC). rTMS focuses specifically on the DLPFC, whereby indirectly stimulation of the sgACC is also achieved transsynaptically as we demonstrated before using Heart-Brain Coupling 2). For psychotherapy, it is thought that among other areas, it also activates the deeper sgACC in this network more directly. Concurrent application of both techniques thus activates a larger part of this malfunctioning ‘depression network’, with higher clinical efficacy.
References:
>1) Donse, L., Padberg, F., Sack, A. T., Rush, A. J., & Arns, M. (2017). Simultaneous rTMS and psychotherapy in major depressive disorder: Clinical outcomes and predictors from a large naturalistic study. Brain Stimulation. doi: https://doi.org/10.1016/j.brs.2017.11.004
2) Iseger, T. A., Padberg, F., Kenemans, J. L., Gevirtz, R., & Arns, M. (2017). Neuro-Cardiac-Guided TMS (Heart-Brain Coupling): Probing DLPFC-sgACC-vagus nerve connectivity using heart rate-first results. Brain Stimulation. doi: http://dx.doi.org/10.1016/j.brs.2017.05.002
Association between ADHD and intensity of sunlight
Association between ADHD and intensity of sunlight: Can ADHD be prevented?
Nijmegen, October 21st, 2013 – A study published today in Biological Psychiatry (Do Sunny Climates Reduce ADHD?) sheds new light on the increasing rates (prevalence) of attention-deficit/hyperactivity disorder, known as ADHD. Children with ADHD have problems with inattention, distractibility, disorganization, impulsiveness, and overactivity. This study found that “sunny” regions with high solar intensity, such as the US states of California, Arizona, and Colorado, and countries like Spain and Mexico have lower prevalence of ADHD. An apparent protective effect of sunlight accounted for 34-57% of the variance in ADHD prevalence. The authors speculate that this may be related to sunlight’s effects on preventing circadian rhythm (“biological clock”) disturbances. These results suggest ways to prevent or treat ADHD for a substantial sub-group of patients.
Researchers from Utrecht University, Research Institute Brainclinics, Leiden University, and Ohio State University today published their work suggesting a possible preventive effect of sunlight on ADHD. Examining ADHD prevalence rates per US state (CDC data, see figure 1a) and solar intensity maps (NREL data, see figure 1b) the authors observed a striking geographical coincidence between low ADHD prevalence and high solar intensity. Solar intensity is a measure of how much sunlight a specific area receives (in kWh/m2/day), often used for calculating how much energy solar panels will generate.
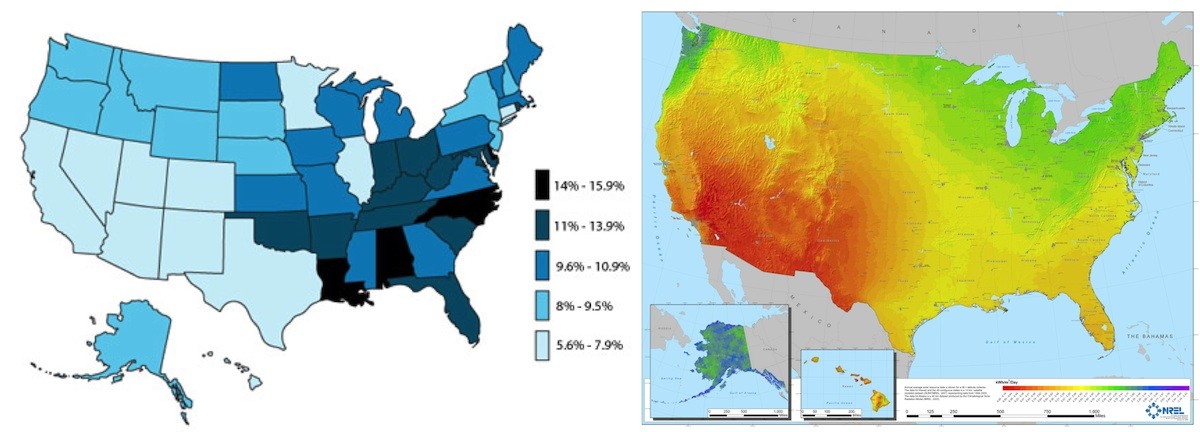
Figure 1a: ADHD Prevalence (CDC, 2003) Figure 1b: Solar-Intensity (NREL)
Based on this initial observation, the researchers further investigated this in 2 US and one non-US datasets, where they found a clear negative dose-response effect between solar intensity and the prevalence of ADHD. Considering all data, solar intensity accounted for 34-57% of the variation in ADHD prevalence. Many potential confounding factors were adjusted for in their analysis such as socio-economic status, low birth weight, infant mortality, geographical latitude, ethnicity/race, etc. However, these factors could not explain the results.
ADHD and sleep
Many patients with ADHD suffer from sleep problems, most often a difficulty falling asleep (or sleep-onset insomnia). For more information also see Sleep and ADHD. Shorter sleep duration and sleep restriction are associated with attention problems. The authors suggest that sleep disturbances may explain the attention problems in this subgroup of ADHD patients. Difficulty falling asleep has been linked to circadian rhythm problems (disturbances of the biological clock) and a delayed melatonin response. It is well known that sunlight is the strongest influence on the human biological clock. The authors hypothesize that this delayed circadian rhythm and difficulty falling asleep may be caused by increased evening use of modern media, such as tablet computers and smart phones, especially with social media increasing the exposure to such blue-light* sources during the evening. The authors speculate that strong sunlight during the day might reset the biological clock and act as an antidote to the evening exposure to artificial blue light causing sleep onset problems. The implications of these findings are that future research in ADHD should take into account sleep and circadian issues. From the public health perspective, manufacturers of tablets, smartphones and PCs could investigate the possibility of time-modulated color-adjustment of screens, to prevent unwanted exposure to blue light in the evening (e.g. f.lux software). Finally, these results could point the way to prevention of a sub-group of ADHD, by increasing the exposure to natural light during the day in countries and states with low solar intensity. For example, skylight systems in classrooms and scheduling playtime in line with the biological clock could be explored further.
* It is known that only 464-484 nm blue light specifically affects the biological clock, incandescent lamps have a low proportion of light in this range, whereas screens and some LED lights have a higher proportion in this range.
Reference: Arns, M. van der Heijden, K.B., Arnold, L.E. & Kenemans, J.L. (2013) Geographic variation in the prevalence of ADHD: The Sunny perspective. Biological Psychiatry DOI: 10.1016/j.biopsych.2013.02.010